Children – 6 months
to 16 years
Tongue tie doesn't resolve as a child grows. Beyond infancy, its impact shifts — from feeding to speech, from speech to eating and breathing, from breathing to sleep quality and dental development. If your child's symptoms have not been fully explained, specialist assessment may provide answers.
Tongue tie in children — beyond the early weeks
Most parents associate tongue tie with breastfeeding difficulties in newborns. But tongue tie doesn't resolve when feeding improves or when breastfeeding stops. The structural restriction remains, and as a child grows, its impact shifts — from feeding to speech, from speech to eating texture, from eating to breathing patterns, from breathing to sleep quality and dental development.
Many children in this age group were assessed in infancy and told their tongue tie was not significant, or not assessed at all. Some had a release as a newborn that addressed feeding difficulties at the time, but the functional restriction was never fully resolved. Others have been through speech therapy, seen orthodontists, or been investigated for sleep disturbance — without anyone identifying the underlying restriction as a contributing factor.
If your child has any of the presentations listed on this page and has not had a specialist tongue tie assessment, it is worth seeking one. We will give you an honest clinical opinion on whether restriction is functionally relevant in your child's case.
Recognise your child's symptoms?
Tongue tie presents differently at every developmental stage. Select the symptom most relevant to your child for a detailed explanation of how it relates to oral restriction and what assessment involves.
- Child · Speech Speech problems and articulation →
- Child · Eating Fussy eating and chewing difficulty →
- Child · Breathing Mouth breathing and open mouth posture →
- Child · Sleep Snoring and poor sleep →
- Child · Dental Dental crowding and orthodontic concerns →
- All ages · Missed diagnosis Tongue tie missed in infancy →
- All ages · Revision Previous release that didn't work →
Our approach for this age group
Our approach for children aged six months and older is different from that used for younger infants. There are four stages to the pathway, and each stage is clinically important — the procedure is not the entirety of treatment.
Initial Assessment
The initial assessment appointment is a comprehensive clinical evaluation — nothing surgical takes place at this visit. One of our chartered physiotherapists will assess your child's oral function first, looking at how the tongue moves, evaluating range and pattern of motion, and identifying any functional compensations that have developed. This is a gentle, unhurried process and we work to ensure your child is comfortable throughout.
This is followed by a medical consultation and examination with Dr. Justin Roche, Consultant Paediatrician. Where clinically appropriate, measurements and clinical photographs may be taken as part of the clinical record. At the end of the appointment we discuss our findings in full. If we identify a functionally significant restriction, we explain what we found and what treatment would involve. If we do not find clinically significant restriction, we tell you that too. We do not recommend treatment unless we are confident it is indicated.
You are not committing to any procedure by attending for assessment. The findings and clinical advice from this appointment have value regardless of whether you proceed further.

What to expect on assessment day
Your child will not require sedation or anaesthetic at the assessment visit. The physiotherapy assessment involves observing tongue movement and is a gentle process. The medical examination follows, and the full appointment ends with a clinical discussion where we explain what we found and what, if anything, we recommend.
If your child is anxious about medical appointments or has had difficult previous experiences, please contact us before your appointment. We are experienced in working with anxious children and can advise on how to prepare them.
Nothing surgical happens at the assessment appointment.
Pre-operative Myofunctional Therapy
In the weeks before surgery, our clinical team works with your child to prepare the tongue and surrounding musculature for the procedure and for the movement patterns that will follow it. This phase is not a preparatory formality — it is a clinically important part of the outcome.
A tongue tie causes structural restriction, and over time the tongue adapts to that restriction, developing compensatory movement patterns that become habituated. Before we release the restriction, we work to begin normalising movement, improving muscle strength and stamina, and introducing the tongue to the range of motion it will have access to post-procedure. This means that when the restriction is released, the functional patterns needed to consolidate the improvement are already being established.
For older children and teenagers, this phase also builds cooperation with the exercises required post-operatively, making the transition to rehabilitation more straightforward. In some cases the pre-operative therapy phase provides information that refines our surgical planning — the extent to which function improves with preparation informs how much of the restriction is structural versus habituated. We work with you to find practical, age-appropriate ways to integrate these exercises into your child's daily routine.

Functional Frenuloplasty under Conscious Sedation
Surgery for tongue, lip, or buccal tie is performed under conscious sedation. This means that although your child will be breathing independently throughout, they will have no memory of the procedure. They are kept comfortable by local anaesthetic applied to the base of the tongue. Throughout the procedure and for a period afterwards, your child is monitored using an ICU-grade monitoring system.
For a child-friendly approach, EMLA numbing cream is applied to the skin 40 minutes ahead of inserting the cannula for IV access. Your child will only be brought to the procedure room after the first dose of sedation has been administered — they will not be distressed by being separated from you during the procedure itself.
Because your child is conscious during surgery, we are able to elicit tongue movements and assess tone in real time. This allows us to gauge more precisely how much fibrous tissue requires release for optimal function, while creating minimal inflammation during healing. The doctor and physiotherapist work together in surgery to ensure all tension has been released. The surgical site is closed with absorbable sutures, which means there is no active wound management required at home post-operatively, minimising discomfort during recovery.
This approach is what differentiates functional frenuloplasty from a release performed under general anaesthetic, where the patient is fully unconscious and muscles are flaccid — precluding the real-time functional assessment that informs precision.

Post-operative Rehabilitation
The period following surgery is where the functional gains of the procedure are consolidated. The release has created the structural possibility for normal tongue movement — the rehabilitation work establishes it as a functional reality.
In the weeks after surgery, our therapy team works with your child on active rehabilitation of the tongue, jaw, and surrounding musculature. This includes continued myofunctional exercises to develop the range, strength, and precision of tongue movement, as well as physiotherapy to address any residual tension in the jaw, neck, and fascial system associated with the restriction.
We also monitor wound healing during this period. The absorbable sutures mean no wound management is required at home, but we assess the surgical site at follow-up to ensure healing is progressing well and that exercises are being performed correctly. Children and families who engage consistently with the post-operative programme achieve significantly better functional outcomes than those who focus on the procedure alone.
For older children and teenagers with habituated compensatory speech patterns, we recommend continued collaboration with your child's speech and language therapist during the post-operative period. We are happy to liaise with your child's SLT directly where this is helpful.

Common questions from parents
If you don't find what you are looking for here, our free Concerns Call is the best next step.
Is there an age limit for treatment?
There is no upper age limit. We treat children from six months through to adolescence, and adults beyond that. The approach and the extent of pre-operative preparation varies with age, but age alone is not a barrier to assessment or treatment.
My child had a tongue tie release as a baby. Can they be reassessed?
Yes, and we see this regularly. A release in infancy may have resolved the immediate feeding concern without fully addressing the functional restriction. As the child grows and the demands on oral function increase, the residual restriction can become more clinically apparent. We will assess the current functional status and advise accordingly.
Will my child need to be put to sleep for the procedure?
We use conscious sedation, not general anaesthetic. Your child will be breathing independently throughout and will have no memory of the procedure. This approach avoids the risks associated with general anaesthesia and allows us to assess tongue movement and tone during surgery, which improves precision. Your child is only brought to the procedure room after the first dose of sedation has been administered, so they will not be distressed by separation during the procedure itself.
How many appointments will we need?
The full pathway involves an initial assessment, a series of pre-operative therapy appointments, the procedure itself, and post-operative follow-up. The number of pre-operative sessions varies depending on the degree of compensatory adaptation and how quickly your child progresses through the preparation exercises. We will give you a realistic expectation of the timeline at the assessment appointment.
Will treating tongue tie fix my child's speech?
If restricted tongue mobility is a functionally significant contributor to your child's speech difficulties, addressing the restriction creates the structural possibility for correct sound placement. The sounds still need to be learned and established through speech therapy and myofunctional rehabilitation. We work in partnership with your child's SLT where one is involved, and we are clear about realistic expectations from the outset. Frenuloplasty is the foundation, not the complete treatment.
My child is anxious about medical appointments. How do you manage this?
We are experienced in working with children who are anxious or who have had difficult previous medical experiences. The assessment appointment involves no procedures and we take as much time as needed. For the procedure, the approach we use — including EMLA numbing cream prior to IV access and administration of sedation before your child enters the procedure room — is specifically designed to minimise distress. Please contact us before your appointment to discuss any specific concerns and we can advise on how best to prepare your child.
My child has been discharged from speech therapy with ongoing difficulties. What should we do?
If your child has persistent articulation difficulties after a course of speech therapy, a specialist tongue tie assessment should be sought if it has not already been completed. We see many children in this situation, and in a significant number a functionally relevant restriction is identified that was not previously considered.
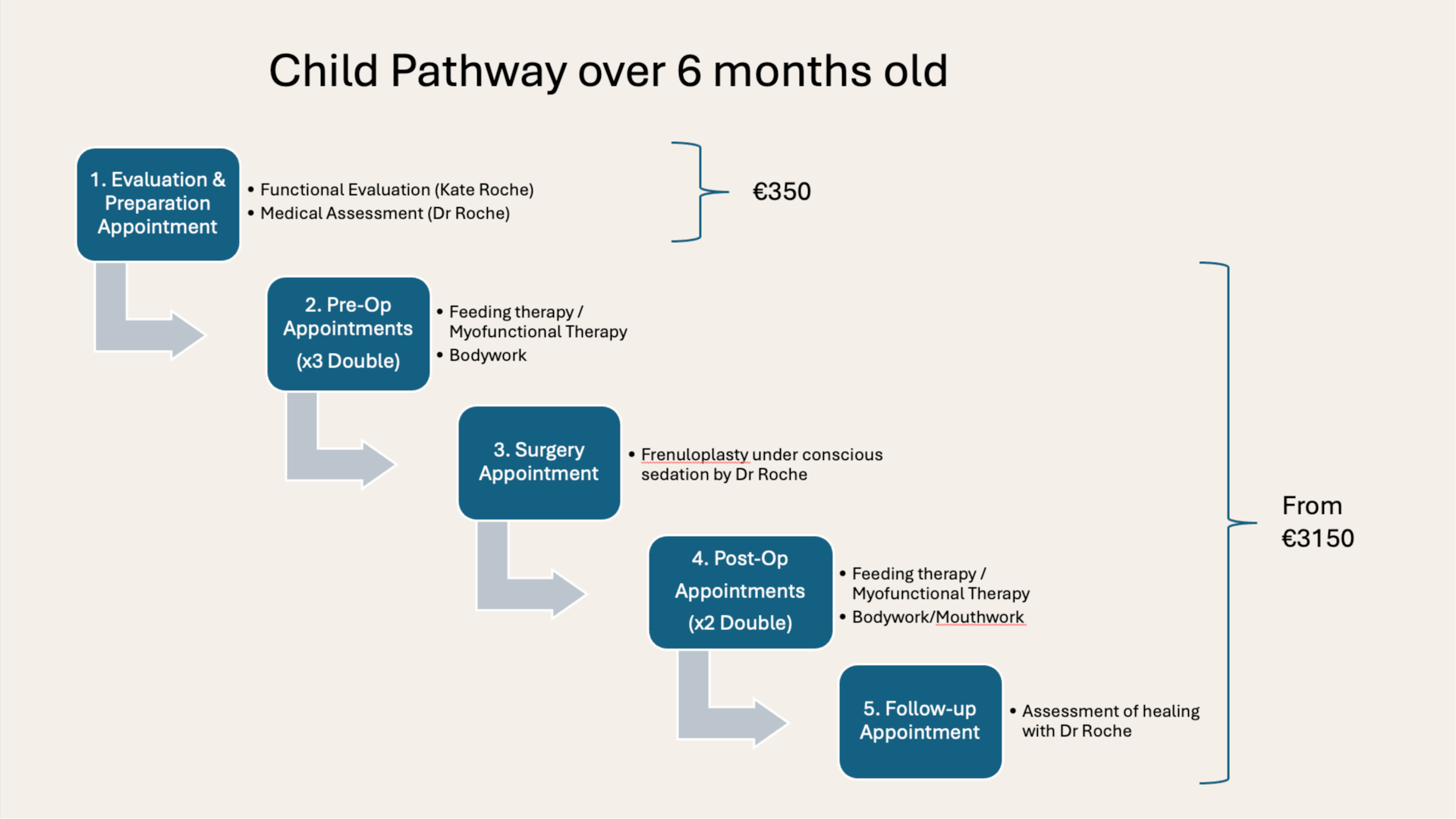
Transparent fee structure
We want to be transparent about cost before you commit to assessment. The initial evaluation is a standalone clinical appointment — you are not obligated to proceed further, and the findings and advice from this appointment have value regardless of whether you go on to the full pathway.
Evaluation and preparation appointment. Standalone clinical visit. No obligation to proceed.
Pre-operative therapy, frenuloplasty under conscious sedation, and post-operative rehabilitation.
A payment plan is available. If you hold private health insurance, please see our fees page for information on what may be covered under your policy. Contact us if you need documentation to support a claim.
Ireland's original dedicated tongue tie clinic
Established in 2007 as Ireland's first clinic dedicated entirely to the assessment and treatment of tongue tie. Led by Dr. Justin Roche (Consultant Paediatrician, FRCPCH, FRCPI, IBCLC) and Kate Roche (Chartered Physiotherapist, IBCLC, Feeding Therapist). Clinics in Clonmel, Co. Tipperary and Naas, Co. Kildare.
Ready to get answers for your child?
If you have been managing your child's symptoms without resolution, or if you have been told that tongue tie is not significant and something still doesn't feel right, a specialist assessment will give you a clear clinical picture. We will tell you honestly what we find and what, if anything, we recommend.
Clinics in Clonmel, Co. Tipperary and Naas, Co. Kildare. Patients seen from across Ireland and internationally.
Frenuloplasty is a surgical procedure. Risks, benefits, and individual expectations are discussed in full at assessment before any decision to proceed is made.
